How Neurofeedback Supports Neurodegenerative Patients
June 30, 2026


Neurofeedback is a non-invasive brain training technique that helps patients with neurodegenerative diseases improve cognitive and motor symptoms by training specific brainwave patterns. Clinically, it is also called EEG biofeedback, and the two terms are used interchangeably throughout this guide. Research shows it benefits patients with conditions ranging from Parkinson’s disease to mild cognitive impairment (MCI), with measurable gains in motor control, memory, and emotional regulation. Understanding how neurofeedback supports neurodegenerative patients gives you a clearer picture of what this therapy can realistically offer and how to pursue it effectively.
Neurofeedback works by giving your brain real-time information about its own electrical activity, then rewarding it for shifting toward healthier patterns. Sensors placed on your scalp read brainwave frequencies. A computer translates those readings into audio or visual feedback, such as a tone or a video that plays smoothly when your brain hits a target pattern. Over repeated sessions, the brain learns to sustain those healthier states on its own.
The physiological effects go deeper than simple conditioning. Neurofeedback increases BDNF (brain-derived neurotrophic factor) and promotes dendrite growth in areas critical for neurodegenerative recovery, including the hippocampus. BDNF is essentially a survival signal for neurons. Higher BDNF levels mean more neurons survive and form new connections, which is exactly what a degenerating brain needs.

Neurodegenerative conditions each produce recognizable brainwave signatures. Parkinson’s disease generates excess beta oscillations in the subthalamic nucleus, which disrupts movement initiation. Alzheimer’s disease and MCI typically show excess slow-wave activity (theta and delta) and reduced upper-alpha power, which correlates with memory and attention deficits. Neurofeedback targets these specific patterns directly.
Clinicians use quantitative EEG, or QEEG brain mapping, to build a precise picture of each patient’s dysfunctional brainwave activity before designing a protocol. This step separates effective neurofeedback from generic approaches. Without a QEEG, a clinician is guessing at which frequencies to train.
Key brainwave targets used in neurodegenerative protocols include:
Pro Tip: Ask any neurofeedback provider whether they use QEEG mapping before starting. If the answer is no, the protocol is not personalized to your brain, and results will be less predictable.
The evidence base is growing, and the 2026 research picture is more encouraging than it was five years ago. Studies are still largely pilot-scale, but the findings are consistent enough to draw meaningful conclusions.
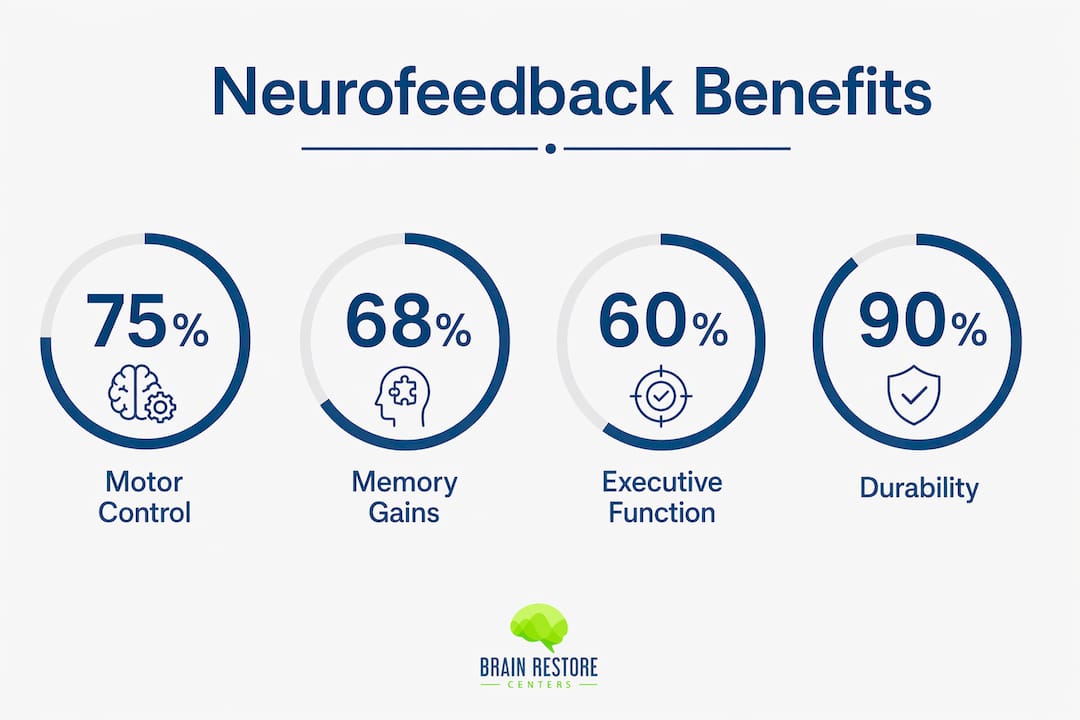
Patients with Parkinson’s showed improvements in motor control, working memory, and logical reasoning after 20 sessions of infra-low frequency neurofeedback. Each session ran 30 minutes, and participants ranged in age from 50 to 95. That age range matters because it shows the therapy is not limited to younger or higher-functioning patients.
For MCI, the evidence is particularly strong on durability. Memory and executive function gains from neurofeedback training were sustained at one-year follow-up in sham-controlled randomized trials. One year of sustained benefit from a non-pharmacological intervention is a meaningful clinical outcome.
EEG neurofeedback protocols can train older adults to shift brainwave activity toward patterns associated with improved attention and memory. This is not a passive process. Patients actively participate in each session, which itself builds cognitive engagement over time.
| Condition | Protocol type | Outcomes reported | Durability |
|---|---|---|---|
| Parkinson’s disease | Infra-low frequency, 20 sessions | Motor control, working memory, logical reasoning | Reported post-treatment |
| Mild cognitive impairment | Upper-alpha, SMR, theta suppression | Memory, executive function | Sustained at 1-year follow-up |
| Cognitive aging | Upper-alpha up-training, gamma exploration | Attention, memory encoding | Ongoing research |
| Parkinson’s (DBS context) | Beta-oscillation modulation | Movement initiation, subthalamic regulation | Pilot findings |
Systematic reviews confirm that effect sizes vary widely, ranging from 0.3 to 1.3 depending on diagnosis and protocol. That range tells you something important: the quality of the protocol and the fit between patient and treatment drive outcomes more than the technology itself.
Not every patient responds equally to neurofeedback, and the field is honest about this. Researchers call low-responding patients “non-responders,” and identifying them before treatment begins is an active area of investigation. Neurophysiological biomarkers are being studied as predictors of who will benefit most, which will eventually allow clinicians to screen patients more accurately.
One finding challenges a common assumption. Cognitive impairment in Parkinson’s is associated with enhanced modulation of subthalamic beta-oscillations during neurofeedback. In plain terms, some patients with cognitive impairment actually show better brainwave modulation capacity than cognitively normal patients. Disease-related network changes may create a therapeutic window that does not exist in a healthy brain.
Personalized protocols built on QEEG data address this variability directly. A precision framework targets upper-alpha, SMR, or mu-suppression based on each patient’s specific map, with dynamic adjustments as the brain responds. This is not a one-size-fits-all approach.
Key factors that shape protocol design include:
Pro Tip: If you are told neurofeedback is not suitable because your cognitive impairment is too advanced, ask for the evidence. Research suggests cognitive deficits do not necessarily preclude a strong training response.
Neurofeedback is best used as an adjunctive treatment, not a replacement for conventional medical care. Effect sizes are real, but neurofeedback does not halt neurodegeneration. It supports the brain’s ability to compensate, adapt, and function better within the constraints of the disease.
Neurofeedback produces its strongest results when it is part of a broader plan. The brain does not operate in isolation from the body, and neither should your treatment. Combining neurofeedback with physical and lifestyle therapies creates synergistic effects that no single modality achieves alone.
Combining neurofeedback with hyperbaric oxygen therapy and laser therapy enhances brain healing through increased oxygenation and reduced neuroinflammation. Hyperbaric oxygen raises oxygen delivery to compromised brain tissue. Laser therapy (photobiomodulation) reduces cellular inflammation and supports mitochondrial function. Together, these therapies address the biological environment in which neurofeedback training takes place.
A practical brain health strategy for neurodegenerative patients typically includes:
High clinical success occurs when neurofeedback is integrated into comprehensive brain health plans that include nutrition, physical therapies, and lifestyle changes. This is not a passive therapy you receive and forget. Active engagement between sessions, including sleep hygiene, movement, and stress management, directly affects how well your brain consolidates the training.
Working with a clinician who specializes in neurodegenerative conditions is non-negotiable. A generalist neurofeedback provider may lack the QEEG expertise and disease-specific protocol knowledge needed to produce meaningful results for Parkinson’s or MCI patients.
Neurofeedback supports neurodegenerative patients most effectively when QEEG-guided personalized protocols are combined with complementary therapies, consistent lifestyle practices, and specialized clinical oversight.
| Point | Details |
|---|---|
| QEEG mapping is foundational | Personalized brainwave maps drive protocol design and predict which frequencies to target. |
| Clinical evidence is real but variable | Effect sizes range from 0.3 to 1.3; protocol quality and patient fit determine outcomes. |
| Cognitive impairment is not a barrier | Some patients with cognitive deficits show stronger brainwave modulation than cognitively normal patients. |
| Adjunctive use maximizes results | Neurofeedback works best alongside conventional care, exercise, nutrition, and complementary therapies. |
| Durability is achievable | Memory and executive function gains from MCI protocols have been sustained at one-year follow-up. |
I have watched neurofeedback move from a fringe curiosity to a credible clinical tool over the past decade. The research trajectory is clear: this therapy works, but it works best when the clinician knows exactly what they are doing with a QEEG and a disease-specific protocol.
What I find most compelling is the finding that cognitive impairment may actually enhance modulation capacity in some Parkinson’s patients. That flips the conventional assumption on its head. Clinicians who dismiss neurofeedback for patients with moderate cognitive decline may be denying them one of the therapies they would respond to best.
The honest limitation is that neurofeedback is not a cure. No clinician should frame it as one. What it offers is a meaningful improvement in quality of life, a way to reclaim cognitive function that felt lost, and a non-pharmacological tool that works with the brain’s own plasticity. For patients navigating a neurodegenerative diagnosis, that is genuinely significant.
My practical advice: do not pursue neurofeedback in isolation. Pair it with a functional medicine evaluation, address your sleep and inflammation, and find a provider who uses QEEG mapping as a standard part of their intake. The therapy is only as good as the plan it sits inside.
— Chad
At Brainrestoremeridian, neurofeedback is one part of a fully integrated brain health program designed for patients facing cognitive and neurological challenges. Every program begins with QEEG brain mapping to build a precise picture of your brain’s activity before a single training session starts.
From there, personalized neurofeedback programs are paired with photobiomodulation, functional medicine, and other restorative therapies to address the full biological picture. The clinic’s team in Meridian, Idaho, specializes in conditions like Parkinson’s, MCI, and cognitive decline, bringing both clinical depth and genuine care to every patient. If you are ready to explore what a personalized brain health plan could look like for you, Brainrestoremeridian is a strong place to start that conversation.
Neurofeedback, also called EEG biofeedback, is a non-invasive brain training method that teaches the brain to shift toward healthier electrical patterns. It is used as an adjunctive treatment for conditions like Parkinson’s disease and mild cognitive impairment.
Yes. Randomized controlled trials show memory and executive function gains from neurofeedback training in MCI patients that were sustained at one-year follow-up. Results depend heavily on protocol personalization and session consistency.
Clinical studies on Parkinson’s patients used 20 sessions of 30 minutes each as a standard course. The exact number varies by diagnosis, QEEG findings, and individual response, and most patients require ongoing monitoring and protocol adjustments.
Neurofeedback is non-invasive and well-tolerated across a wide age range, including patients aged 50 to 95 in published studies. Cognitive impairment does not preclude treatment and may in some cases predict a stronger training response.
Research confirms that integrated brain health plans that include neurofeedback alongside nutrition, physical therapies, and lifestyle changes produce the highest clinical success rates. Neurofeedback alone is less effective than neurofeedback within a comprehensive care strategy.

